Pathophysiology
COPD
COPD is characterized by chronic bronchitis, emphysema, and inflamed airways. Emphysema is the abnormal enlargment of airspaces due to the destruction of alveolar wall tissue. Bronchitis is characterized by the inflammation of the bronchioles leading to hypertrophy and fibrosis of the respiratory smooth muscle, accompanied by mucosal gland enlargement and ciliary abnormalities. In the case of COPD, inflammation refers to increased oxidative stress, increased levels of proteases with decreased levels of antiproteases, as well as inflammation due to irritants such as cigarette smoke.
Asthma
IgE mediated mast cell activation leads to the release of histamine, tryptase, leukotrienes, and prostaglandins leading to bronchoconstriction and vasodilation. Over the following hours, TH2 lymphocytes are activated, leading to the release of interleukins and GM-CSF, which results in mucosal hyper secretion, goblet cell proliferation, and eosinophilic infiltration of lung tissue. Excessive immune activation also leads to some fibrosis of the airway. Lastly, due to chronic activation, smooth muscle hypertrophy is exhibited.
Diagnosis and Staging
COPD
S/Sx
- Chronic Cough
- Dyspnea
- Increased Sputum Production
- Increased RR
- Use of Accessory Muscles to Breath
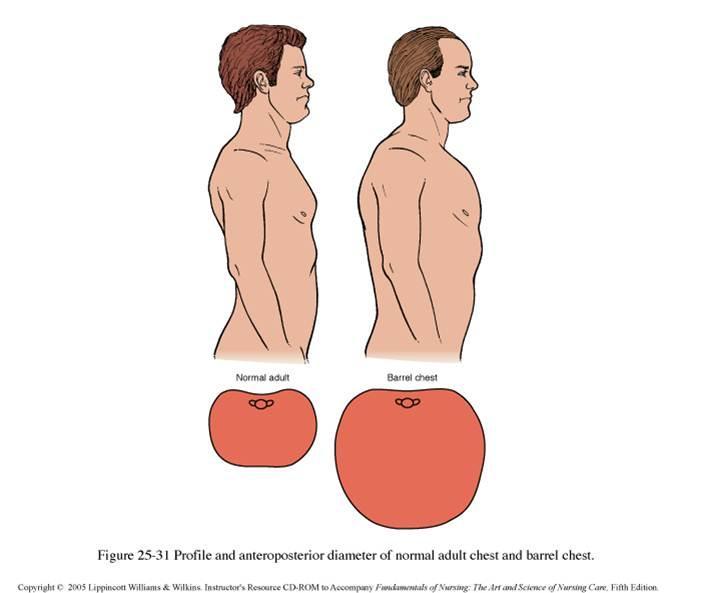
- Barrel Chest
- Decreased Breath Sounds
- Prolonged Exertion
Risk Factors
- Smoking
- Genetics
- Age
- Hx of Asthma or other Reactive Airway Diseases
- Respiratory Infections
- FHx
Dx
Spirometric Assessment with FEV1/FVC < 0.7
Staging
Symptomatic Assessment
| Stage | Symptomatic Assessment | Exacerbations |
|---|---|---|
| A | CAT < 10 OR mMRC ≤ 1 | ≤1 |
| B | CAT ≥ 10 OR mMRC ≥ 2 | ≤1 |
| C | CAT < 10 OR mMRC ≤ 1 | ≥2 OR ≥1 Hospitalization |
| D | CAT ≥ 10 OR mMRC ≥ 2 | ≥2 OR ≥1 Hospitalization |
Spirometric Airway Limitation
| Stage | Impairment | FEV1 / FVC | FEV1 |
|---|---|---|---|
| GOLD 1 | Mild | <0.7 | ≥80% Predicted |
| GOLD 2 | Moderate | <0.7 | [50%,80%) Predicted |
| GOLD 2 | Severe | <0.7 | [30%,50%) Predicted |
| GOLD 3 | Very Severe | <0.7 | <30% Predicted |
mMRC Grading
| mMRC Grade | Severity of Breathlessness |
|---|---|
| 0 | SOB w/ Strenuous Exercise |
| 1 | SOB w/ Moderate Exertion (e.g. walking uphill or walking quickly) |
| 2 | SOB w/ Normal Activity (e.g. cannot keep up with others or must stop at normal pace) |
| 3 | SOB w/ Mild Activity (Walking for <100m) |
| 4 | Cannot leave the house, SOB w/ dessing/undressing |
Asthma
SSx
- Chest-tightness
- Dyspnea
- Non-productive cough
- Wheezing
Dx
- Reversible airway obstruction w/ bronchodilators
- Elevated IgE and eosinophils
Staging
| Intermittent | Mild-Persistent | Moderate-Persistent | Severe-Persistent | |
|---|---|---|---|---|
| SSx Frequency | ≤ 2d / week | > 2x / week | Daily | Multiple times / day |
| Nighttime Awakening | ≤ 2x / month | 3-4x / month | > 1x / week | ≥ 7x / week |
| SABA Use | ≤ 2d / week | > 2x weekly & < 1 QD | Daily | Multiple times / day |
| Interference w/ Normal Activity | None | Minor | Some | Severe |
| Lung Function Tests | FEV1 > 80% FEV1 / FVC Normal |
FEV1 > 80% FEV1 / FVC Normal |
FEV1 [60%, 80%) FEV1 / FVC Reduced 5% |
FEV1 < 80% FEV1 / FVC Reduced 5% |
| Exacerbations Requiring PO Steroids | 0-1 | ≥ 2 | ≥ 2 | ≥ 2 |
Treatment
COPD
Maintenance Therapy
| GOLD Group | 1st Line | 2nd Line |
|---|---|---|
| A | Bronchodilator | Try Another Class |
| B | LABA | LABA + LAMA |
| C | LAMA | LABA + LAMA |
| D | LABA + LAMA | LABA + LAMA + ICS |
GOLD C can conider a LABA + ICS combination for second line therapy; however it is not as effective. GOLD D can consider Roflumilast if FEV1 < 50% predicted w/ chronic bronchitis, and macrolide Abxs can be considered for former smokers.
COPD Exacerbations
Treatment
- Albuterol w/ or w/o Ipratropium
- Prednisone 40mg PO QD x5d
- Abx
- Macrolides, Amoxicillin/Clavulantate, or Tetracyclines x5-7d
- Indicated w/ Ventilator Use or w/ Purulent Sputum and either Increased Sputum Volume or Dyspnea
- Can provide supplemental O2
- Consider non-invasive ventilation before intubation
- **If exacerbation pt is intubated and crashing, disconnect vent circuit, as respiratory arrest due to breath-stacking is very common
- Monitor Lung function annually
Discharge Criteria
- SABA not needed more than q4h
- Pt can cross room if they could at baseline
- Pt can eat and sleep w/o frequent awakening
- Clinically stable for 12-24hr
Prevention / Non-Pharm
- Provide O2 to increase O2Sat to > 90%
- Smoking cessation
- Vaccination
- Flu
- Pneumococcal
- Transplant
Asthma
Maintenance Therapy
- Therapy proceeds in a stepwise manner
- Start low, titrate as necessary
- Below is general therapy level necessary for control
- Intermittent: Step 1
- Mild: Step 2
- Moderate: Step 3-4
- Severe: Step 5-6
- Step down if controlled for 3mo but do not eliminate ICS
| Step 1 | Step 2 | Step 3 | Step 4 | Step 5 | Step 6 | |
|---|---|---|---|---|---|---|
| Reliever | PRN SABA | PRN SABA | PRN SABA | PRN SABA and Low-Dose ICS / Formoterol | PRN SABA and Low-Dose ICS / Formoterol | PRN SABA and Low-Dose ICS / Formoterol |
| Preferred Control Agent | None | Low ICS | Low ICS / LABA | Med or High ICS / LABA | Add Tiotropium, Anti-IgE, or Anti-IL5 | Add low-dose PO GC |
| Alt Control Agents | Low ICS | Leukotriene Modifier Theophylline |
Med / High ICS Low ICS + LT Modifier Add Theophylline |
Add Tiotropium High ICS + LT Modifier Add Theophylline |
Add low-dose PO GC Consider Omalizumab |
Consider Omalizumab |
Status Asthmaticus
- PO or IV GCs
- 2 mg/kg prednisone equivalents QD NTE 60 mg QD
- Intermittent SABA / SAMA in ED
- O2 to ≥ 90%
- Fluid resuscitation if necessary
- Consider non-invasive ventilation before intubation
- **If exacerbation pt is intubated and crashing, disconnect vent circuit, as respiratory arrest due to breath-stacking is very common
- Second Line
- Switch from intermittent to continuous SABA
- Albuterol 0.5 mg/kg/hr NTE 20 mg/hr
- Monitor HR & K
- MgSO4 25-75 mg/kg IV x1 dose NTE 2 g/dose
- Switch from intermittent to continuous SABA
- Third Line
- Terbutaline
- Monitor BP, HR, K
- Aminophylline / Theophylline
- Monitor HR / Rhythm, and plasma conc
- Minimal evidence
- Ketamine
- Heliox
- Volatile Anesthetics
- Terbutaline
Prevention / Non-Pharm
- Avoid NSAIDs
- Vaccinate
- Flu
- Pneumococcal if ≥ 19yo
- Regular exercise
Common Inhalers
| Brand Name | Active Ingredient(s) | Class(es) |
|---|---|---|
| ProAir, Ventolin, Proventil | Albuterol | SABA |
| Xopenex | Levalbuterol | SABA |
| Atrovent | Ipratropium | SAMA |
| Combivent | Albuterol / Ipratropium | SABA / SAMA |
| QVAR | Beclomethasone | ICS |
| Pulmicort | Budesonide | ICS |
| Alvesco | Ciclesonide | ICS |
| Aerospan | Flunisolide | ICS |
| Flovent, ArmonAir | Fluticasone Propionate | ICS |
| Arnuity | Fluticasone Furoate | ICS |
| Asmanex | Mometasone | ICS |
| Brovana | Arformoterol | LABA |
| Foradil | Formoterol | LABA |
| Arcapta | Indacaterol | LABA |
| Striverdi | Olodaterol | LABA |
| Servent | Salmeterol | LABA |
| Tudorza | Aclidinium | LAMA |
| Spiriva | Tiotropium | LAMA |
| Incruse | Umeclidinium | LAMA |
| Advair, AirDuo | Fluticasone / Salmeterol | ICS / LABA |
| Symbicort | Budesonide / Formoterol | ICS / LABA |
| Dulera | Mometasone / Formoterol | ICS / LABA |
| Breo | Fluticasone / Vilanterol | ICS / LABA |
| Stiolto | Olodaterol / Tiotropium | LABA / LAMA |
| Anoro | Vilanterol / Umeclidinium | LABA / LAMA |
| Utibron | Indacanterol / Glycopyrronium | LABA / LAMA |
| Bevespi | Formoterol / Glycopyrronium | LABA / LAMA |
SEs
- β-Agonists
- Skeletal muscle tremors
- Palpitations
- Tachycardia
- Hypokalemia
- Hyperglycemia
- Boxed warning for increased risk of Asthma-Related death was removed in 2018 ADD CITATION HERE
- Anticholinergics
- Dry mouth
- Dizziness
- Blurred vision
- Urinary retention
- URIs
Guidlines
References
- Barrel Chest Image Available at https://ratedmedicine.wordpress.com/barrel-chest/