Formulas 1
General PK
1-Compartment Model
Vancomycin 1, 2, 3, 4
Peak: 20-40 mg/L
Trough: 10-15 mg/L (minor infections) or 15-20 mg/L (serious infections or lung penetration)
Loading Dose: 25-30 mg/kg (Wt)
NTE 15 mg/min
k ≈ 0.00083 × CrCl + 0.0044
Vd ≈ 0.4-1 L/kg, usually 0.6-0.7 L/kg
for appropriate effect
to prevent toxicity
Initial Vanc Dosing Calculator
Level-Based Vanc Dosing Calculator
Aminoglycosides 1, 5
See also: Stanford Aminoglycoside Dosing Guidelines
k ≈ 0.0024 × CrCl + 0.01
Vd ≈ 0.26 L/kg × Wt
Vd may be closer to 0.3-0.35 L/kg in critically ill pts due to fluid overload
Use ABW if Wt/IBW > 130%
Traditional Dosing
Gentamicin / Tobramycin Target Levels 1, 6
| Infection | Target Peak (mcg/mL) | Target Trough (mcg/mL) |
|---|---|---|
| General | 4-10 | le; 1 |
| UTI | < 5 | ≤ 1 |
| Bacteremia | > 5 | ≤ 1 |
| Pneumonia | > 6 | ≤ 1 |
| Endocarditis from P. aeruginosa | > 12 | ≤ 1 |
| Infection | Target Peak (mcg/mL) | Target Trough (mcg/mL) |
|---|---|---|
| General | 15-30 | 4-10 |
| UTI | > 15 | 4-10 |
| Bacteremia | > 20 | 4-10 |
| Pneumonia /Serious Infections | > 24 | 4-10 |
Target Cpk / MIC > 10 for efficacy Draw levels 1hr after infusion ends Consider target troughs of ≤ 1.5-2 (tob/gent) or ≤ 10 (amikacin) for life-threatening infections. Look up specific trough/peak targets for given infection site.
Initial Aminoglycoside Dosing Calculator
Extended-Interval Dosing
-
Load with 7 mg/kg (15 mg/kg Amikacin)
-
Determine initial dosing frequency from table below
-
Draw level at 6-14hr after 1st or 2nd dose
-
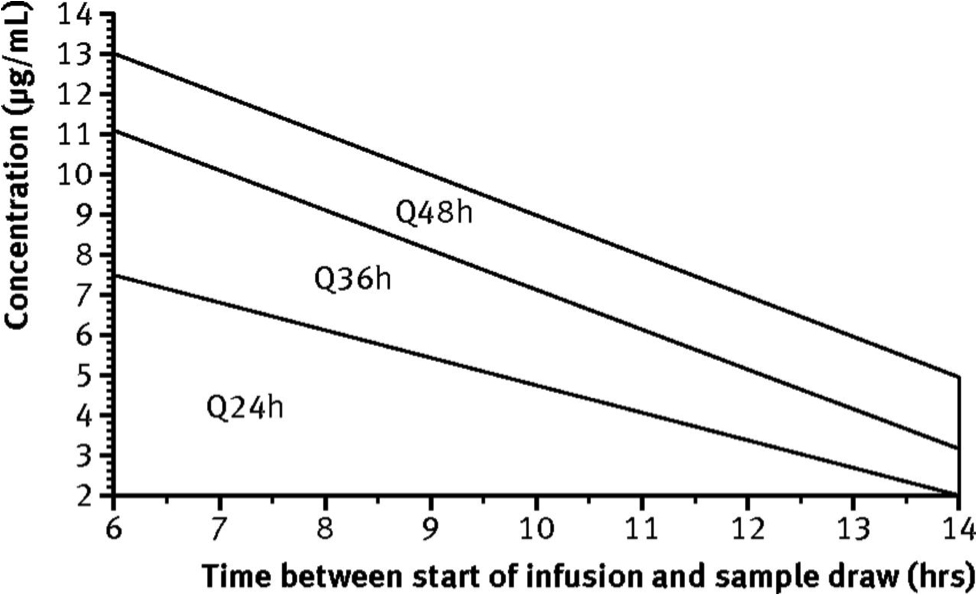
Plot level on Hartford Nomogram (divide level by 2 for Amikacin)
- If doses other than those above are used, multiplying the level by (expected)/(given) dose can help adjust properly for the nomogram, although this has less evidence
-
Adjust interval per nomogram
-
If borderline, go with longer interval
Hartford Nomogram
Initial Aminoglycoside Interval
| CrCl | Interval |
|---|---|
| ≥ 60 | Q24H |
| 40-59 | Q36H |
| 20-39 | Q48H |
| < 20 | Monitor Serial Conc. & Admin when < 1 mcg/mL |
References
-
DiPiro JT, ed. Pharmacotherapy: A Pathophysiologic Approach. Tenth edition. New York: McGraw-Hill Education; 2017. ↩ ↩2 ↩3 ↩4 ↩5
-
Rybak M, Lomaestro B, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. American Journal of Health-System Pharmacy. 2009;66(1):82-98. doi:10.2146/ajhp080434 ↩
-
Matzke GR, McGory RW, Halstenson CE, Keane WF. Pharmacokinetics of vancomycin in patients with various degrees of renal function. Antimicrobial Agents and Chemotherapy. 1984;25(4):433-437. doi:10.1128/AAC.25.4.433 ↩
-
Deryke CA, Alexander DP. Optimizing Vancomycin Dosing through Pharmacodynamic Assessment Targeting Area under the Concentration-Time Curve/Minimum Inhibitory Concentration. Hospital Pharmacy. 2009;44(9):751-765. doi:10.1310/hpj4409-751 ↩
-
Nicolau DP, Freeman CD, Belliveau PP, Nightingale CH, Ross JW, Quintiliani R. Experience with a once-daily aminoglycoside program administered to 2,184 adult patients. Antimicrobial Agents and Chemotherapy. 1995;39(3):650-655. doi:10.1128/AAC.39.3.650 ↩
-
Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Riverwoods, IL. Available at: http://online.lexi.com. ↩ ↩2